
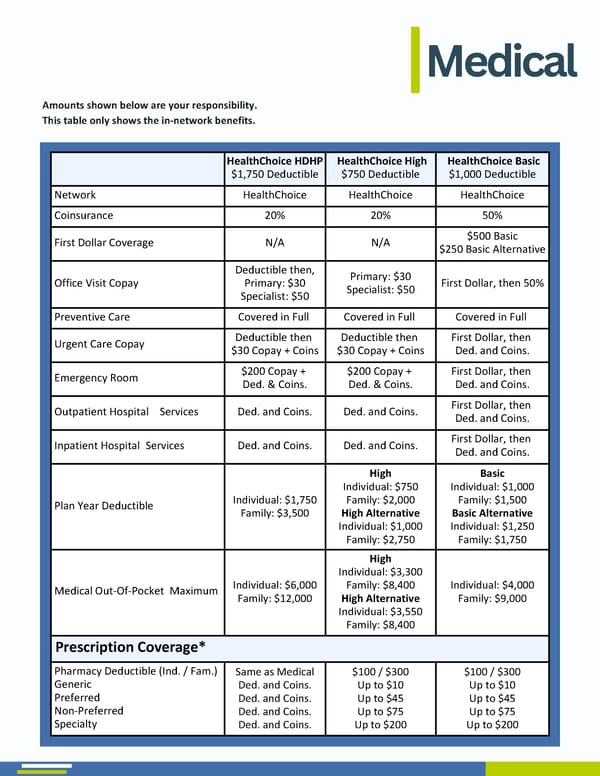
Medical Amounts shown below are your responsibility. This table only shows the in-network benefits. HealthChoice HDHP $1,750 Deductible HealthChoice High $750 Deductible HealthChoice Basic $1,000 Deductible Network HealthChoice HealthChoice HealthChoice Coinsurance 20% 20% 50% First Dollar Coverage N/A N/A $500 Basic $250 Basic Alternative Office Visit Copay Deductible then, Primary: $30 Specialist: $50 Primary: $30 Specialist: $50 First Dollar, then 50% Preventive Care Covered in Full Covered in Full Covered in Full Urgent Care Copay Deductible then $30 Copay + Coins Deductible then $30 Copay + Coins First Dollar, then Ded. and Coins. Emergency Room $200 Copay + Ded. & Coins. $200 Copay + Ded. & Coins. First Dollar, then Ded. and Coins. Outpatient Hospital .Services Ded. and Coins. Ded. and Coins. First Dollar, then Ded. and Coins. Inpatient Hospital .Services Ded. and Coins. Ded. and Coins. First Dollar, then Ded. and Coins. Plan Year Deductible Individual: $1,750 Family: $3,500 High Individual: $750 Family: $2,000 High Alternative Individual: $1,000 Family: $2,750 Basic Individual: $1,000 Family: $1,500 Basic Alternative Individual: $1,250 Family: $1,750 Medical Out-Of-Pocket .Maximum Individual: $6,000 Family: $12,000 High Individual: $3,300 Family: $8,400 High Alternative Individual: $3,550 Family: $8,400 Individual: $4,000 Family: $9,000 Prescription Coverage* Pharmacy Deductible (Ind. / Fam.) Generic Preferred Non-Preferred Specialty Same as Medical Ded. and Coins. Ded. and Coins. Ded. and Coins. Ded. and Coins. $100 / $300 Up to $10 Up to $45 Up to $75 Up to $200 $100 / $300 Up to $10 Up to $45 Up to $75 Up to $200
 2026 Benefit Guide MPS Page 4 Page 6
2026 Benefit Guide MPS Page 4 Page 6