
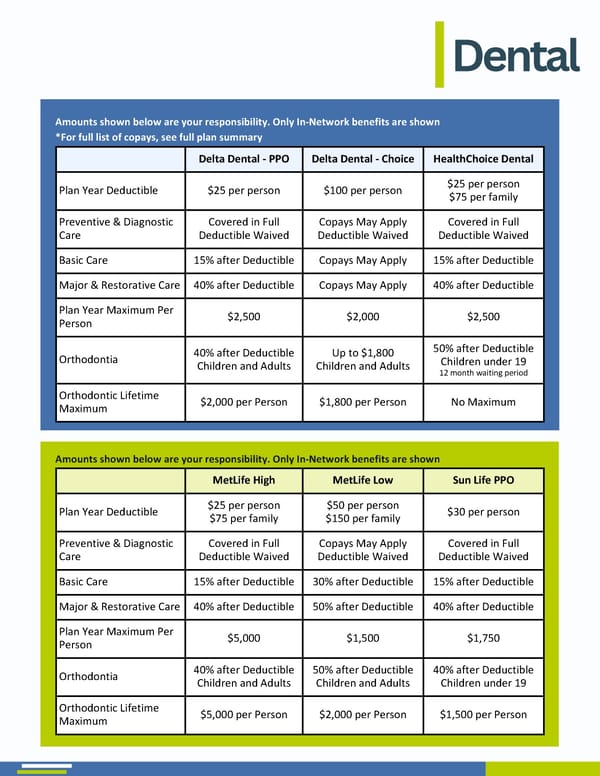
Dental Amounts shown below are your responsibility. Only In-Network benefits are shown *For full list of copays, see full plan summary Delta Dental - PPO Delta Dental - Choice HealthChoice Dental Plan Year Deductible $25 per person $100 per person $25 per person $75 per family Preventive & Diagnostic Care Covered in Full Deductible Waived Copays May Apply Deductible Waived Covered in Full Deductible Waived Basic Care 15% after Deductible Copays May Apply 15% after Deductible Major & Restorative Care 40% after Deductible Copays May Apply 40% after Deductible Plan Year Maximum Per Person $2,500 $2,000 $2,500 Orthodontia 40% after Deductible Children and Adults Up to $1,800 Children and Adults 50% after Deductible Children under 19 12 month waiting period Orthodontic Lifetime Maximum $2,000 per Person $1,800 per Person No Maximum MetLife High MetLife Low Sun Life PPO Plan Year Deductible $25 per person $75 per family $50 per person $150 per family $30 per person Preventive & Diagnostic Care Covered in Full Deductible Waived Copays May Apply Deductible Waived Covered in Full Deductible Waived Basic Care 15% after Deductible 30% after Deductible 15% after Deductible Major & Restorative Care 40% after Deductible 50% after Deductible 40% after Deductible Plan Year Maximum Per Person $5,000 $1,500 $1,750 Orthodontia 40% after Deductible Children and Adults 50% after Deductible Children and Adults 40% after Deductible Children under 19 Orthodontic Lifetime Maximum $5,000 per Person $2,000 per Person $1,500 per Person Amounts shown below are your responsibility. Only In-Network benefits are shown Amounts shown below are your responsibility. Only In-Network benefits are shown *For full list of copays, see full plan summary
 2026 Benefit Guide MPS Page 5 Page 7
2026 Benefit Guide MPS Page 5 Page 7